The amendments to the International Health Regulations and the new Pandemic Treaty and what they will mean for YOU!
Last updated: 4 February 2024
The WHO is the World Health Organisation, an agency of the United Nations (UN) that is responsible for international public health.
Both organisations are currently preparing 4 documents that purport to be treaties or accords and all in the name of health and future pandemics. These documents are being drafted under urgency, behind closed doors, by unelected officials.
They are a mixture of new treaties and amendments to 2005 International Health Regulations, which New Zealand is already bound.
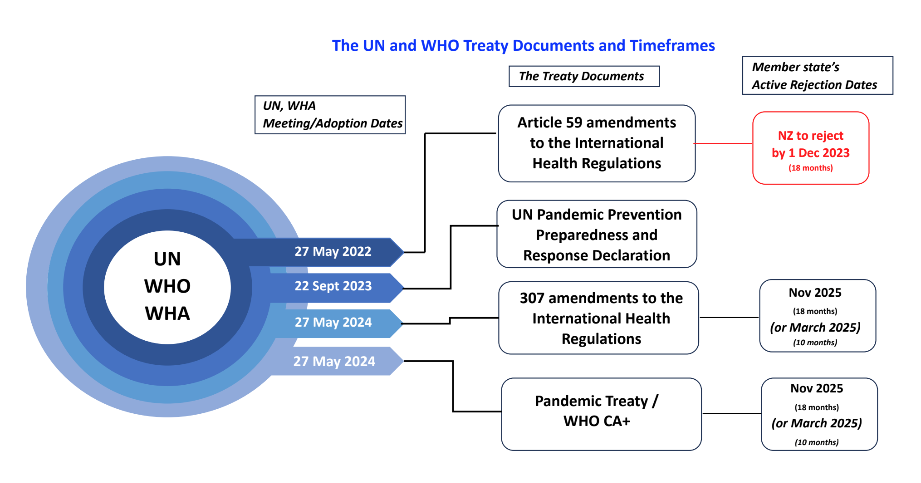
The 4 treaties are:
- The new UN’s Political Declaration of the United Nations General Assembly Pandemic, Prevention, Preparedness and Response Manifesto – zero draft (UN PPPR Declaration)
- Article 59 amendments to the International Health Regulations (Article 59 IHRAs)
- 300+ draft amendments to the International Health Regulations (300+ IHRAs)
- A new pandemic instrument called the Pandemic Treaty or WHO CA+ (Pandemic Treaty)
The 4 treaties will hand the WHO the authority to make binding directions on how a country is required to respond to a potential public health emergency (not necessarily an actual one). Under the treaties, the WHO will be able to order measures including significant financial contributions from individual Member States, censor scientific debate, order lockdowns, restrict travel, force medical examinations and mandatory vaccinations, all in the name of health.
Whatever your views of the Covid pandemic, we can all agree that before running headlong into new and more rules, that the more appropriate step for the UN and the WHO would be to stop and reflect, hold hearings and make findings on what worked, what didn’t and what could have been done differently.
Upcoming Important Dates include:
- 27 January 2024: The 300+ IHRAs were required to be delivered to the Member States in accordance with the WHO’s own rules [this has not happened and the date has now passed].
- End May 2024: 77th World Health Assembly at which the 300+ IHRAs and Pandemic Treaty will likely be adopted.
- March 2025: Member States will have to reject any adopted amendments (300+ IHRAs).
- May 2025: Member States will have to implement into domestic law any adopted amendments (30o+ IHRAs).
- Nov 2025: Member States will have to have implemented or rejected provisions in the the new WHO CA+.
Following is more details on each of the 4 treaties and other information about the WHO and UN, including, most importantly, what you can do!
Table of Contents
Table of Contents
- What can YOU do about the WHO?
- Who’s the WHO, the WHA and the UN?
- Who’s funding the WHO?
- What are the UN and the WHO up to? The 4 treaties and the timeframes.
- What’s the hurry? And why in secrecy?
- The UN’s Pandemic Prevention, Preparedness and Response Declaration
- The WHO’s treaty documents – review and commentary
- WHO’s amendments to the International Health Regulations: Art 59 IHRAs; and 300+ IHRAs
- Pandemic Treaty/WHO CA+
- What are our Ministers telling us?
- Additional Helpful Resources
1. What can YOU do about the WHO?
The most common thing we hear when we mention to anyone that the UN and the WHO are amending and creating pandemic treaties is: “Why haven’t I heard about this?”
This response goes for everyone, from MPs, to public servants and your everyday person on the street.
Clearly media also doesn’t know as they too would be reporting on the potential effects these changes may have on us – wouldn’t they?
So absent anyone knowing, it’s our job to talk about it and to take action:
- Get informed. Talk to people, ask them if they’re aware of the international vaccine pass requirements – anticipated for implementation globally by all Member States, possibly as early as March 2025. Invite them to check out this web page.
- The Government is calling for feedback, ecourage people to provide feedback on both the Pandemic Treaties: Here
- Provide your feedback on the 300+ IHRAs by 18 February 2024, we have helped with some templates: Here
- Provide your feedback on the new Pandemic Treaty: Here
- Write to our new Government and your local MPs. Better yet, go and meet them. Their email addresses are: HERE
VFF has been very active on this topic. Katie our head of legal has appeared before the US, AU and NZ governments regarding what the WHO is proposing and the likely impact.
It’s up to all of us to get informed and talk about what is going on! So let’s start talking.
2. Who’s the WHO, the WHA, and the UN?
The WHO is the World Health Organisation, an agency of the United Nations (UN) responsible for international public health.
The UN, is an intergovernmental organisation whose stated purposes are to maintain international peace and security, develop friendly relations among nations, achieve international cooperation, and serve as a centre for harmonising the actions of nations. It is the world’s largest international organisation. The UN is made up of 194 Member States and its work are guided by the purposes and principles contained in its founding Charter.
The UN says: “it remains the one place on Earth where all the world’s nations can gather together, discuss common problems, and find shared solutions that benefit all of humanity.”

The WHO is governed by the World Health Assembly (WHA), which is the decision-making body of the WHO. Meetings of the WHA are held annually in May. The WHA is attended by delegations from all 194 Member States and focuses on a specific health agenda prepared by the Executive Board (made up of 34 health specialists). The main functions of the WHA are to determine the policies of the WHO, appoint the Director-General of the WHO, supervise financial policies, and review and approve the proposed programme budget.
The WHO says it is: “Dedicated to the well-being of all people and guided by science, the World Health Organization leads and champions global efforts to give everyone, everywhere an equal chance to live a healthy life.”
We understand that the WHO is a longstanding organisation that has in the past been responsible for many good deeds for health the world-over. However, there are some things that the WHO is less well known for: things which might not cast the organisation in the best light.
Furthermore, now, with large portions of the WHO’s funding coming from private organisations/donors and countries with ‘ideals different from established concepts of democracy’ (ie China, North Korea, Russia), there are strong commercial and political interests which influence the decisions made under the proposed treaties and amendments.
New Zealand has been a member of the WHO since 1946. New Zealand was one of the founding countries “and participated in the International Health Conference in 1946, which resulted in the drafting of the WHO constitution, turning over the functions of the Office International d’Hygiene Publique (OIHP) to WHO and setting up of an Interim Commission to prepare for the First World Health Assembly.”
By virtue of its membership to the WHO, New Zealand is bound without reservation to the International Health Regulations of 1968 and the amendment of 2005 (2005 IHRs).



3. Who’s funding the WHO?
At its inception in 1948, the WHO was an independent organisation funded by the 61 founding Member states and many members of government still believe this to be the case.
Unfortunately, the integrity of the WHO has been undermined over time, as industrial donors asserted their influence through the corporate and public/private funding mechanism via Voluntary Contributions. As many of us have come to understand in recent years, it is easy to recognise an organisation’s power and its allegiances if one takes time to look at how it is being funded.
What’s the WHO’s budget?
The WHO’s total approved budget for 2020–2021 is over US$7.2 billion and for 2022-2023 is US$ 6.72 billion.
For the two yearly period for 2020-2021, the WHO received the following funding:
- Assessed contributions from Member States $956M
- Voluntary contributions from Member States $5.824B
- Voluntary contributions – Thematic $513M
- Core Voluntary contributions $236M
- PIP Contributions $51M
Where does the WHO’s funding come from?
In the 2020-2021, the WHO’s top contributors were Germany and the European Commission led donations with US$ 1.734 billion, followed by Gates-dominated enterprises with US$ 1.183 billion, and the United States with US$ 693 million.
China is the 11th largest donor with a contribution of US$ 168 million but holds significant geopolitical influence, including within the WHA.
- Assessed contributions (AC) derive from a percentage of the gross domestic product of each member state (country) and cover less than 20% of the total WHO budget.
- Voluntary contributions (VC) come from Member States, private companies and organisations, and are often termed Public Private Partnerships (PPPs). PPPs account for over 80% of the WHO’s budget. Major private contributors are primarily the Bill and Melinda Gates Foundation and the Gates-funded GAVI Alliance.
Breaking down the Voluntary Contributions further:
Nearly 90% of the voluntary contributions are earmarked to specific programs and locations, meaning they are tied to the preferences of the donors.
Margret Chan, the previous Director-General of the WHO said about fundraising:
“I have to take my hat and go around the world to beg for money and when they give us the money [it is] highly linked to their preferences, what they like. It may not be the priority of the WHO, so if we do not solve this, we are not going to be as great as we were.” (Franck 2018)
The Bill & Melinda Gates Foundation is alone responsible for over 88 per cent of the total amount donated by private donors. Many people are unaware of the sway this foundation holds over the WHO by virtue of its donations. Bill Gates’ biennial contributions of $4.84 billion dollars through the Bill & Melinda Gates Foundation exceeded that of any member state.
This unprecedented platform for influence has not gone unnoticed, and in 2017 Politico was prompted to say of Bill Gates:
“He is treated like a head of state, not only at the WHO, but also at the G20.”
…
“His sway has NGOs and academics worried. Some health advocates fear that because the Gates Foundation’s money comes from investments in big business, it could serve as a Trojan horse for corporate interests to undermine WHO standards and shaping health policies.”
The WHO’s own webpage boasts:
“Investment in WHO returns major benefits to its investors. These investors are taxpayers and citizens the world over. They can be assured that their investment in WHO is being returned many times over. The world needs WHO to be “financially fit for purpose” so that it can “deliver on its broad – and ever-growing – mandate to act as the world’s leading authority on global health.”
Dr David Bell, an Australian clinical and public health physician with a PhD in population health and former WHO scientific and medical officer, says the following about the WHO’s funding:
“The WHO was established in 1946 with the best of intentions, to help coordinate responses to major health issues and advise governments accordingly. Over the decades we have seen a significant change in direction as funding streams have shifted to private “specified funding”, particularly from private donors. This has led to the WHO becoming a far more centralised and externally-directed body in which private and corporate funders shape and direct programmes.”
We must all be aware of and concerned about the commercial interests and ultimate persuasions that have infiltrated the WHO.
4. What are the UN and the WHO up to?
The 4 Treaties and the timeframes
In 2022, during the Covid-19 response, in unison, the UN prepared its UN PPPR Declaration and the WHA handed down a Decision to commence reworking the 2005 International Health Regulations (2005 IHRs) and draft a new pandemic treaty in the name of strengthening Pandemic Prevention, Preparedness and Response.
This has seen the creation of four separate documents which have been described as declarations, treaties, or accords.
1. The UN PPPR Declaration, which was tentatively adopted at the High-level Meeting on 20 September 2023.
2. The WHO’s proposed amendments to the 2005 International Health Regulations (IHRAs) have been intentionally split into two parts:
These amendments appeared minor in number. Yet they were significant in that they greatly reduced the timing to reject future amendments (from 18 months to 10 months) and the requirement to implement (from 24 months to 12 months).
Fortunately, New Zealand rejected the amendments in time (before 1 December 2023), so as to allow the incoming Government to be able to conduct a National Interest Assessment, which must include assessment of the the 300+ IHRAs currently being drafted.
These are being worked on at present, with the Working Group scheduled to hold two more meetings before May 2024.
On 15 December 2023, the IHR Review Committee was required to reconvene to review the package of amendments agreed to by the Working Group with final technical recommendations are required to be submitted to the WHO’s Director General by end of January 2024, so they can be circulated 4 months in advance of the 77th WHA, where they will likely be adopted.
However, the WHO has failed to comply with its own rules, and the 300+ IHRAs have not been supplied to Member States. The problem with this is that we will have no time to consider the substantial 300+ amendments before we are due to vote on them in May 2024.
3. The WHO’s drafting of a new Pandemic Treaty/WHO CA+, which is currently being worked on at present, with the three more meetings scheduled between now and March 2024. This document requires a 2/3rd majority of votes by Member States for it to be adopted at the 77th World Health Assembly end of May 2024.
Following is a diagram that visually outlines the 4 treaties, their status and the dates which NZ has to actively reject:

5. What’s the hurry? And why in secrecy?
The reasons the UN and the WHO give for the urgent preparation of these documents is:
In recognition of the catastrophic failure of the international community in showing solidarity and equity in response to the coronavirus disease (COVID-19) pandemic…
If this is the justification for the documents currently being drafted, then we should be concerned: following the Covid-19 pandemic, there has been no pause, no stop for reflection on what went wrong and what could be done better. Instead the UN and the WHO are running headlong into amending and preparing new treaty documents all in the name of health. What’s more alarming is that our elected governments are letting them!
Whatever your beliefs, everyone of us can agree that a review on the cost benefits of locking down the healthy, masking children, and population wide vaccination is necessary to confirm whether those extreme measures has left the world a healthier place.
The concern with what is currently being drafted is it is being done on the mistaken belief that the WHO, health departments, and our governments around the world got it right.
Relevantly, the response to the Covid-19 pandemic over the last 4 years was achieved under the existing 2005 IHRs. So any new powers the UN and the WHO bestow upon themselves will give the UN and the WHO inordinate amounts of power over how a Member State manages its own public health crises.
Both the amendments to the 2005 IHR and the new Pandemic Treaty raise significant alarm bells for the sovereignty of Member States, the freedoms of individuals to be able to move freely and make choices for their own health, and it will directly impact upon our ability to move freely around the globe.
These concerns are heightened with the public/private funding received by the WHO and the power the WHO will now have to declare a ‘health risk’ of potential (not actual) concern. Such loose wording means that a ‘health risk’ could extend to climate related issues.
As any amendments to the existing 2005 Regulations, which New Zealand is bound without reservation, require no express or written formal approval to become binding, it is incumbent on us all to ensure that our Government are aware of the 4 treaties and that this is an election issue and we will hold our elected official accountable for any decisions they make.
In order for the amendments to not apply to New Zealand, they have to be expressly rejected by our WHO delegate/representative at either Ministry of Foreign Affairs and Trade or the Department of Health. That representative is appointed to the role. Meaning they are not elected by us, rather they are a public servant (as confirmed by former Prime Minister Hipkins in answer to questions raised by Keri Molloy, outlined in section 10. What are our representatives and Ministers telling us?).

6. The UN’s PPPR Declaration
[Document 1]
The UN’s new Political Declaration of the United Nations General Assembly on Pandemic Prevention, Preparedness and Response – Zero Draft – Manifesto (UN PPPR Declaration) was tentatively adopted at the UN High-Level Meeting late September 2023.
The UN PPPR Declaration has been described by the Global Preparedness Monitoring Board as “a key opportunity for the transformation of the global health ecosystem for PPPR, laying out key requirements for the HLM for which it has since advocated.”
So what’s in the UN PPPR Declaration? Following are just some of the clauses that raise the eyebrow.
1. How much will this cost?
That US$30B will be required annually to be prepared to respond to a health emergency – that is US$30B outside of Official Development Assistance Levels and is only for the WHO to be prepared for a health emergency – it does not mention the amounts required for an actual ‘health emergency’ (PP29 ad OP39):
2. What are we being promised?
The UN PPPR Declaration promises to ensure access for all to pandemic related products, not just the vaccine or therapeutic treatments but also the diagnostic tools (such as the PCR tests), which the UN has offered to coordinate with unspecified ‘relevant partners’, which may be pharmaceutical corporations and vaccine promoting NGOs, Coalition for Epidemic Preparedness Innovations, GAVI the Vaccine Alliance (OP2).
3. What kind of pandemic related products are we promised?
Of note, vaccines are mentioned 17 times in this UN PPPR Declaration. It also calls for improved routine immunisation and vaccination (OP38 (page 12)):
4. Censorship and control of the narrative
The UN/WHO will manage the ‘infodemic’ and control the narrative by quashing any mis and dis-information (OP32 (page 11)):
5. All by May 2024 so they can be voted upon
The UN PPPR Declaration calls for the conclusion of the negotiations of the 300+ IHRAs and Pandemic Treaty at the 77th WHA scheduled for the end of May 2024 (OP44 (page 13)):
Status of the UN PPPR Declaration
The UN PPPR Declaration has only been tentatively adopted because of objections raised by the 11 countries.
The 11 countries were Belarus, Iran, Bolivia, Nicaragua, Cuba, Russia, Korea, Syria, Eritrea, Venezuela, Zimbabwe.
The 11 countries raised concerns about the lack of ‘true and meaningful’ engagement with all member states in the negotiation of the UN PPPR Declaration. The 11 countries also opposed the attempt by the Un President to adopt the declaration at a high level meeting, without the full assembly present (a requirement of the relevant resolution).
Given the status and where the UN PPPR Declaration has progressed to, there is nothing for New Zealand to do with respect to the UN PPPR Declaration at this stage.
7. The WHO’s treaty documents – review and commentary
The WHO is amending the 2005 International Health Regulations and creating a new Pandemic Treaty. They both contain wording that we should all be aware of and open to discuss.
We share the concerns of Dr David Bell, an Australian clinical and public health physician with a PhD in population health and former WHO scientific and medical officer who says:
“the two agreements, as currently drafted, will hand the WHO the authority to order measures including significant financial contributions by individual states, censorship of scientific debate, lockdowns, travel restrictions, forced medical examinations and mandatory vaccinations during a public health emergency of its own declaring.”
David Bell is also not alone in his concerns. The amendments to the 2005 IHRs has been reviewed by the IHR Review Committee. The IHR Review Committee is an Expert Advisory Panel made up of 17 experts and specialists that was established especially for the sole purpose “to provide technical recommendations to the WHO’s Director-General on the 300+ IHRAs”.
In February 2023, a Review Committee considered the 300+ IHRAs. The 20 Review Committee were critical of the 300+ IHRAs pointing out that what was proposed:
- raised “sovereignty concerns” for Member States (Article 12);
- changed the nature of the WHO’s recommendations from “non-binding to binding, and giving a binding effect” (Article 1);
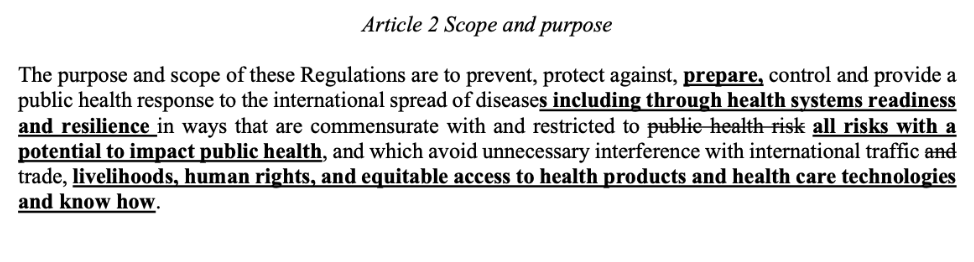
- “replace[d] “public health risk” with “all risks with a potential to impact public health” may not increase the clarity of this Article.”” (Article 2);
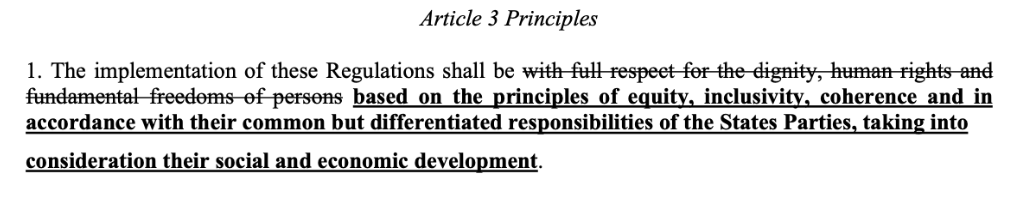
- defied individual human rights with the removal of the words “full respect for the dignity, human rights and fundamental freedoms of persons” as an overarching principle in the first paragraph, and notes that the concepts of human rights, dignity and fundamental freedoms are clearly defined within the framework of treaties to which many of the States Parties to the Regulations have adhered.” (Article 3);
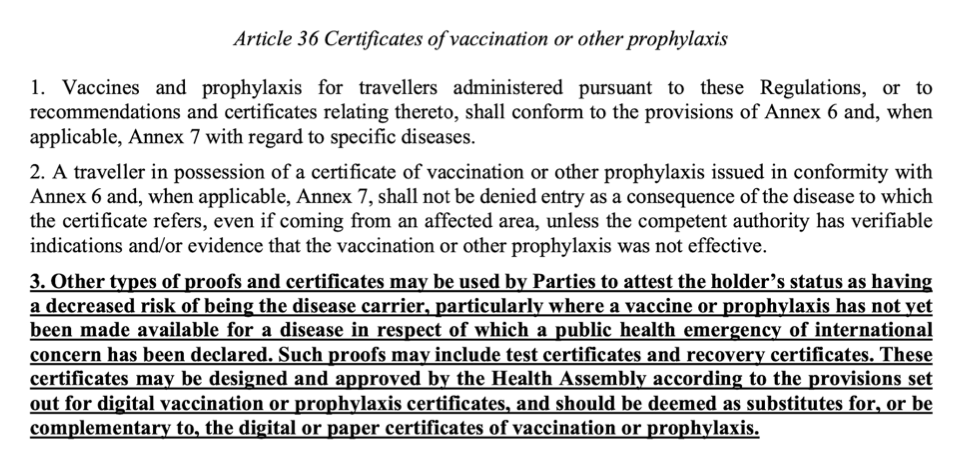
- proposed universal implementation of health/vaccine passports “the Committee is concerned that such a requirement may burden travellers, and may even raise ethical and discrimination-related concerns .” (Articles 23, 35 and 36).
It is unclear whether the IHR Review Committee’s concerns have been considered by the Working Group since we have not seen any further updates on the 300+ IHRAs since they were first released 17 December 2022.
Dr David Bell further concerns reiterate those of the IHR Review Committee:
“the amendments to the IHR … constitute a dangerous increase in power and authority bestowed on just one person. The Director General would be able to proclaim health emergencies, whether real or potential, on any health-related matter that they, influenced by their private and corporate funders, say is a threat. The WHO would be able to issue legally binding directions to member states and their citizens. In light of the catastrophic harms the WHO’s policies have caused during this pandemic, probably greater than the virus itself, the potential economic and health-related harms of such power cannot be overstated. There is a vast pandemic industry waiting for these buttons to be pushed and I am in no doubt that policymakers should reject WHO’s pandemic proposals.”
The 300+ IHRAs are potentially harmful as they:
- Have a Member States cede its sovereignty with respect to health to the WHO
- The WHO’s Director General will be granted the power to proclaim potential, not actual, health emergencies
- The fundamental principle of individual human rights and choices are replaced for the collective concepts of equity, inclusivity and cohesion
- Health or travel passes are squarely on the table
- Member States will be required to supply information to the WHO, and the WHO can chose to use, share or withhold any information it sees fit
Can the WHA and the WHO give themselves this power?
No, of course they can’t. The can only get this power if our government gives it to them!
We are also concerned by what it proposed in the documents, as it appears to be well outside the authority of the World Health Assembly and what it can regulations concerning. The WHO’s Constitution at Article 21 limits the authority to:
“Article 21 The Health Assembly shall have authority to adopt regulations concerning:
(a) sanitary and quarantine requirements and other procedures designed to prevent the international spread of disease;
(b) nomenclatures with respect to diseases, causes of death and public health practices;
(c) standards with respect to diagnostic procedures for international use;
(d) standards with respect to the safety, purity and potency of biological, pharmaceutical and similar products moving in international commerce;
(e) advertising and labelling of biological, pharmaceutical and similar products moving in international commerce.” (emphasis added)
Further, Article 23 of the Constitution makes clear “the WHA only has the authority to make recommendations with respect to any matter within the competence of the Organization.”
What the 300+ propose goes well outside ‘procedures designed to prevent the international spread of disease’.
8. Amendments to the International Health Regulations:
Article 59 IHRAs
300+ IHRAs
300+ IHRAs
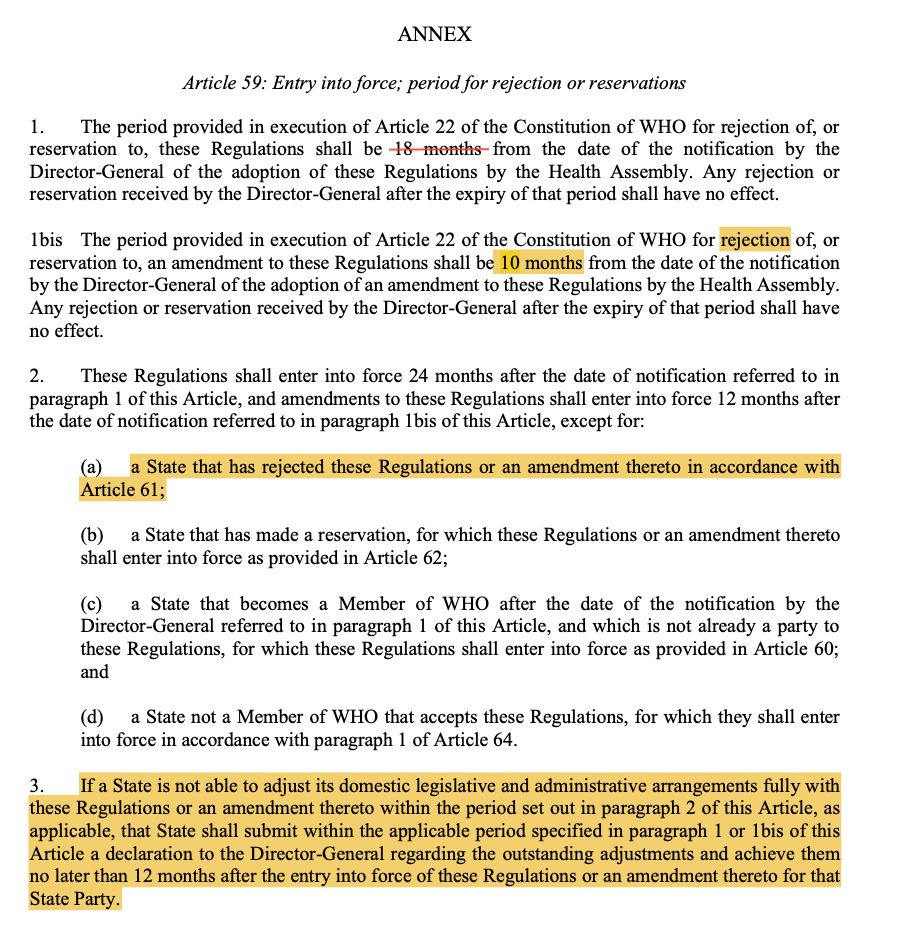
A. The Article 59 IHRAs
This Article 59 IHRAs amend the 2005 IHRs (2005 3rd ED) and were adopted by the WHA on 27 May 2022. They propose reducing the timing for rejection or implementation of any future proposed IHRAs (from 18 to 10 months, and 24 to 12 months respectively):
New Zealand was successful in rejecting the Article 59 IHRAs in time. They were correctly rejected on the basis that the incoming government wished to have a full review of all UN and WHO agreements that were being negotiated and up for consideration. Such documents are now required to be subjected to a National Interest Assessment.
It is our collective hard work that made this an election issue!
Thanks to all that signed The People’s Letter which set out that the Article 59 IHRAs could only be rejected, not reserved! We were right as the government documents confirmed.
B. The 300+ IHRAs:
Remember, we have still only been provided the December 2022 version of the 300+ IHRAs. Since they were first delivered there have been at lease 6 formal meetings of the working group, of which our former Director-General of Health co-chairs alongside Dr Abdullah Asiri of Saudi Arabia.
So what do the 300+ IHRAs say?
1. The WHO’s Standing Recommendations will be binding and the WHO can declare a health emergency if it has potential – it doesn’t have to be an actual health emergency
Under the 300+ IHRAs, the WHO is able to determine an international health concern (of the WHO’s choosing) and that decision and consequential decision about that emergency will have BINDING effect – that is, each Member State must comply with the WHO’s decisions.
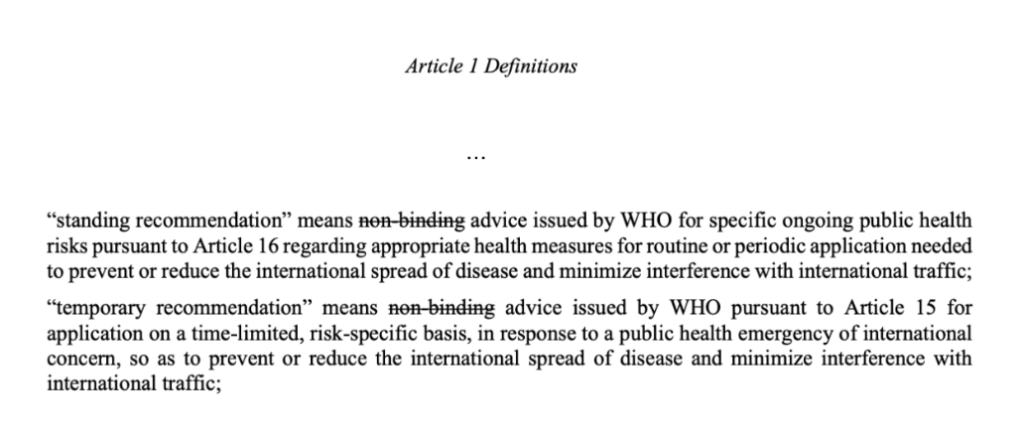
Standing recommendations under the current 2005 IHRs are expressly stated to be “non-binding”, i.e. the WHO’s advice is recommendations or suggestions only – member states can choose to follow the recommendations or not.
The 300+ IHRAs propose deleting the words non-binding in Article 1 inferring that standing recommendations will now be binding. There are other subsequent amendments in Articles 12, 42, 43 that suggest this interpretation is correct, that a member states will be bound to the WHO’s decisions. This is where the concerns arise that New Zealand will lose its sovereignty if the WHO gets to make decisions on our country’s behalf.
In Article 1, the deletion of the word non-binding’ has been deleted, inferring that standing recommendations will be binding:
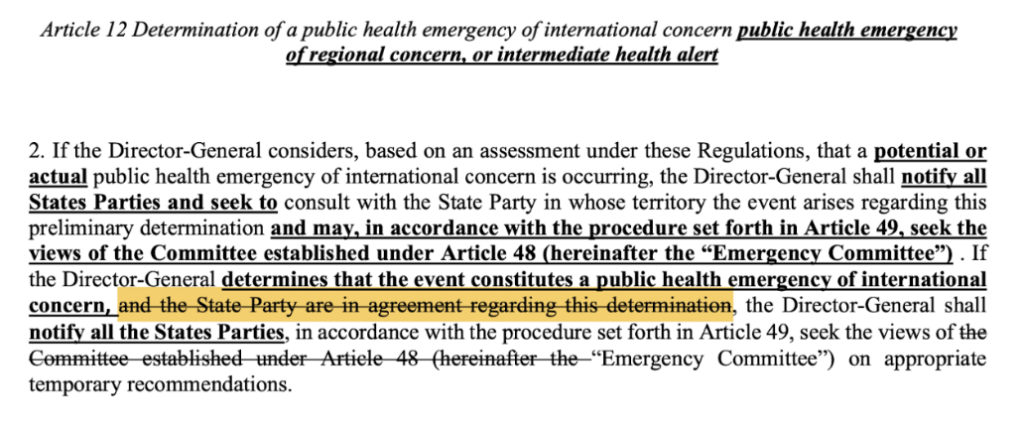
Similar changes proposed in Article 12 provide that if the WHO’s Director-General can determine a potential not actual public health emergency of international concern, and the State Party, in whose territory the event arises no longer has a say whether the Director-General’s determination is appropriate or correct.
Article 12 proposes removing the State Party’s right to agree to the classification of the public health emergency by the WHO Director-General.
Article 42 proposes that the State Party will have to implement the WHO’s recommendations without delay:

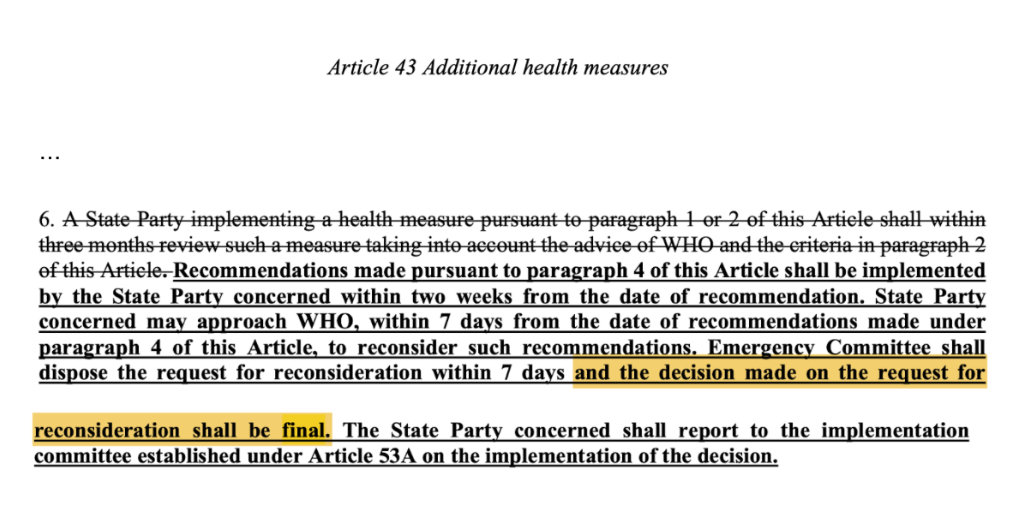
Article 43 grants the Emergency Committee final say on recommendations required to be implemented by a concerned Member State:
The proposed drafting expands the WHO’s scope and purpose for potential, not actual health risks (in Article 2 and see also Article 12 above). The WHO defines any potential health risk of international health concern (of the WHO’s choosing). This wording is so loose and could arguably be used for more than a pandemic (e.g. such health risks could include climate related issues).
2. Removal of individual human rights and choice for common good concepts of ‘equity, inclusivity and coherence’
The WHO’s proposed principles will no longer be around individual human rights but rather equity and coherence. This is likely around the medical response to be adopted to an event, including which pharmaceuticals are to be administered and who is to receive them. See Article 3:
3. Health passports
Digital Passenger Locator Forms will require health passports detail pathogen testing and/or vaccination status. See proposed amendments to Articles 23 and 36:
Work on the digital health passports is already well advanced with the infrastructure being built and installed as you read this. More information regarding the Global Digital Health Certification Network is available:
- WHO’s website, which was supplied by the New Zealand’s Ministry of Health in response to a request: https://www.who.int/initiatives/global-digital-health-certification-network
- WHO’s Global Initiative on Digital Health; and
- The European Commission and WHO launch landmark digital health initiative to strengthen global health security in June 2023.
- The European Parliament and Members States in early November 2024, reached agreement to introduce the Digital Identity.
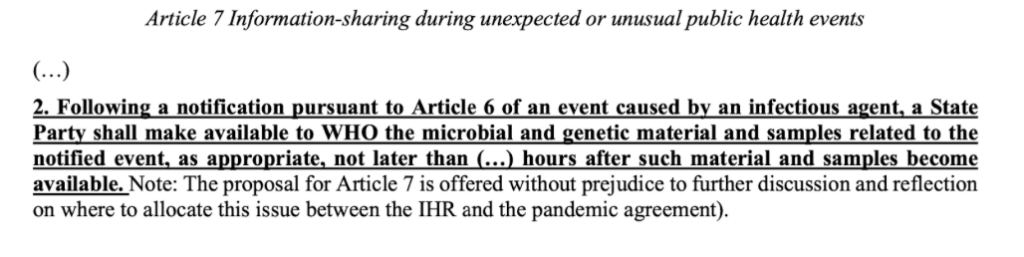
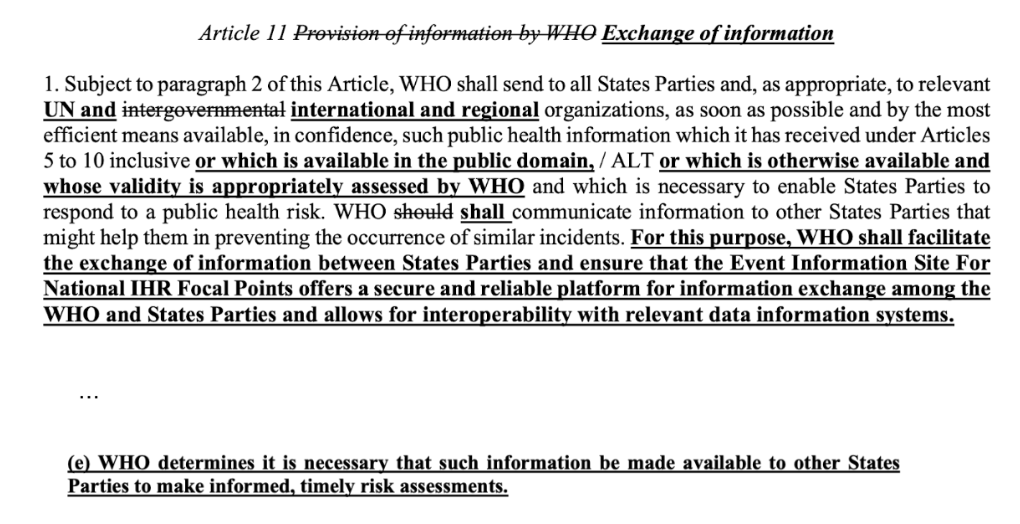
4. The supply of peronal health information to the WHO
Member States will be required to share personal health information to the WHO, and the WHO has the power to share or withhold any information as it sees fit, see Articles 7 and 11:
5. There are a number of other amendments in the current draft of the 300+ IHRAs where:
-
- The WHO may direct Member States give money to developing nations – Article 44A
- A new Compliance Committee is to be established – another new committee but one that ensures Member States are complying with the IHRs – Article 53
- Expands the powers of each member state’s appointed National IHR Focal Point. New Zealand already has an unelected appointed National IFR Focal Point, namely the Office of the Director of Public Health in the Ministry of Health who at present is Dr Nicholas Jones.
Status
The version of the 300+ IHRAs that are publicly available are the ones circulated 17 December 2022.
Much work has been done at numerous meetings since the 300+ IHRs were first supplied.
Decision WHA 75/9 specified that the final version of the 300+ IHRAs was to be circulated to all Member States 4 months in advance of them being voted upon for adoption, which is scheduled for the 77th WHA (end of May 2024).
This makes sense, it gives all Member States a chance to consider the amendments before they are due to vote on them. And given there are in excess of 300 proposed amendments that will significantly change the nature of the IHRs, having plenty of time to consider the changes is vitally necessary. Failure of the WHO to provide the amendments to Member States with sufficient time to consider is a failure of due process and undermines the time honoured rules of fairness and cooperation.
The 300+ IHRAs have not been circulated in accordance with the Decision, in fact the Working Group has further meetings scheduled in February and March 2024 to allow them to continue to work on them. Leaving all Member States in the dark on what they say.
In October 2023, the Working Group indicated that they would not be able to meet the delivery date of mid January 2024. So they obtained advice from WHO lawyer, Stephen Solomon who explained how the Working Group did not need to comply with its own rules. Mr Solomon’s advice is at 27:00 of the October 2024 Working Group meeting.
We view this legal advice as double dutch.
This whole issue with failing to provide the 300+ amendments in accordance with the Decision and rules raises the very real question: if the WHO can’t be trusted to follow its own rules on process, how can it be trusted to follow its own rules re power it is proposing to grant itself under the 300+ IHRAs and Pandemic Treaty?
9. The WHO’s Pandemic Treaty
The Pandemic Treaty is an entirely new document that purports to be a treaty but its latest iteration actually calls it what it is: “Proposal for negotiating text of the WHO Pandemic Agreement”, so an agreement to agree. Hence why it’s also been called the WHO CA+.
The WHO CA+ is an entirely new convention agreement, which establishes a framework for the identification, tracking, collection of pathogens and sets out management of a pandemic and the funding of the WHO and its partners by Member States.
The background explanation set out in the June 2023 version of the WHO CA+ gave the reason for the document:
In recognition of the catastrophic failure of the international community in showing solidarity and equity in response to the coronavirus disease (COVID-19) pandemic, the World Health Assembly convened a second special session in December 2021, where it established an Intergovernmental Negotiating Body (INB) open to all Member States and Associate Members (and regional economic integration organizations as appropriate) to draft and negotiate a WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response, with a view to its adoption under Article 19, or under other provisions of the WHO Constitution as may be deemed appropriate by the INB.
(emphasis added)
These are incredibly powerful and emotive words used to justify the implementation of this convention agreement, especially as there has been no pause for reflection, inquiry or report into the successes and failings of the last 4 years.
The latest version of the WHO CA+ (30 October 2023) has deleted the words above. You can review previous versions of the Pandemic Treaty/WHO CA+ unedited here and the version made publicly available on 12 June 2023 here and 16 October 2023 here.
The Pandemic Treaty/WHO CA+ reads more like a trade agreement than a health treaty. It:
- Sets up an international supply networks which will be overseen by the WHO.
- Outlines the funding structures and processes including Member States to pay ≥5% of their national health budgets, which will be ‘devoted to health emergencies’.
- Sets up a new ‘Governing Body,’ under the auspices of the WHO auspices, to oversee the whole process.
- Expands the scope of the ‘One Health’ agenda.
So what are some of the most worrying things proposed in the Pandemic Treaty/WHO CA+?
1. Equity and inclusivity and the One Health approach
A One Health, approach, as opposed to individual human rights and freedoms to choose are one of the core constructs throughout the proposed documents but clearly articled throughout the Pandemic Treaty/WHO CA+.
See Articles 1 (definition), Article 5, with One Health:

2. Outlines public health surveillance, including to test and collect all sorts of pathogens of pandemic potential and store them in a central location
Article 4:
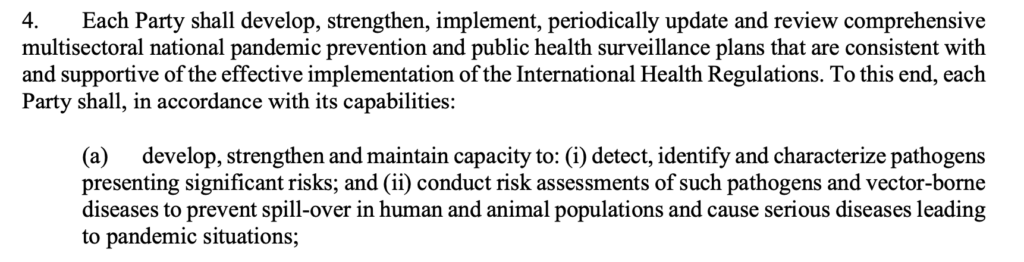


See also Article 1 (l) WHO coordinated laboratory network”, Article 6, 9, 10.
3. Specify the amounts of money Member States must pay the WHO to establish this infrastructure for the WHO
See Article 20 regarding Financing (see part):
5. Control the information and the narrative
It does this by dropping the conditions for public funding of R&D in Article 9, while simultaneously curtailing free speech and also supplying the information. Check out Article 1 definition of infodemic, Article 18 re combating mis and disinformation (sound similar to the proposed Online Censorship Laws being proposed in New Zealand and elsewhere around the world), followed by Article 21 which is a panel of experts who will provide scientific advice.
Article 1 – definition, and Article 18:

Article 24:

6. Limit liability to the vaccine companies through indemnification and establish vaccine injury compensation schemes
The Pandemic Treaty/WHO CA+ under the guise of liability risk management is not proposed for the purposes of fairly compensating the injured, rather to protect the pharmaceutical manufacturers by setting compensation schemes, ensuring indemnity provisions in vaccine supply contracts, reducing liability for ‘pandemic related products and changing the laws of the Member State making the above referred publicly available.

Status
The Pandemic Treaty is anticipated for adoption at the 77th WHA at the end of May 2024.
10. What are our representatives and Ministers telling us?
All these changes being proposed are pretty extensive and all encompassing, so what are our ministers and elected officials telling us?
In March 2023, Prime Minister Hipkins in response to question from journalist Keri Molloy, which she has published on her Substack, had the following to say:
Strengthening the global health architecture for pandemic prevention, preparedness and response (PPPR) is key to ensuring the world does not face a crisis of the same magnitude as COVID-19 again. It is also one of New Zealand’s foremost global health priorities.
Negotiating a new instrument on pandemic prevention, preparedness and response (PPPR) and amending the International Health Regulations (2005) to ensure they are fit for purpose are key processes to achieving this goal, and New Zealand has been actively engaging in both negotiations since their early 2022 and early 2023 respectively.
…
While the exact form of the instrument is yet to be determined, if Member States agree to proceed with a legally binding instrument (for example, a treaty) standard New Zealand treaty-making processes, including Cabinet approval and parliamentary treaty examination, will be required before New Zealand could become party to the treaty.
Unlike New Zealand lawmaking, where elected representatives vote on laws, the WHO lawmaking process involves mostly unelected diplomats voting on the treaty.
…
New Zealand government representatives are participating in negotiations in both the INB and WHR. Any decision to become party to a new treaty will be decided by the government once negotiations are concluded and would be subject to New Zealand’s treaty-making processes, including Cabinet approval, parliamentary treaty examination, and the passing of legislation if required.
As the 300+ IHRAs are amendments and not a new treaty, it was possible the amendments to the IHRs might not be passed through Cabinet’s official parliamentary treaty examination processes. However, since making this an election issue, NZ First and National included in their Coalition Agreement that all UN and WHO Treaties would be subject to a National Interest Test.
It’s now our collective job to make sure they stick to their promises!